Vaginal Mesh
Sydney Urodynamic - Monday, February 10, 2020Pelvic floor disorders such as prolapse and urinary incontinence are common with up to 50% of women being affected at some stage of their life. Prolapse is a condition where pelvic organs, such as the bladder, uterus and rectum, descend abnormally into the vagina. There are many factors that may predispose to prolapse, but childbirth, particularly vaginal deliveries and especially if forceps are required, is the most important. Other factors are ageing, family history, obesity and chronic straining or coughing. When conservative therapy is unsuccessful for these conditions, surgery may be appropriate.

We know that 20% of women who have a prolapse procedure may require a further operation in the future. This is most likely because the original risk factors are still present, such as damage to the pelvic floor muscles in the sense of overstretching or tearing. Gynaecologists have tried to minimise the risk of prolapse recurrence by reinforcing the repair with `mesh’, which is a permanent, woven material made of Polypropylene. The rationale for using this material was that mesh use has dramatically decreased the risk of recurrence in hernia surgery, and vaginal prolapse is essentially a hernia through the pelvic floor muscle and vagina. Medical studies have in fact shown that using mesh in prolapse repairs can decrease the risk of prolapse recurrence, particularly when used to treat bladder prolapse (also known as cystoceles), and especially in women with pelvic floor muscle tears.
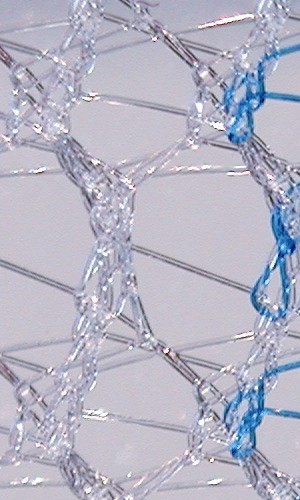
Polypropylene mesh
It is estimated up to 180,000 women in Australia have had a transvaginal mesh procedure for urinary incontinence or prolapse. The majority of procedures have been performed for urinary stress incontinence. However, there has been controversy in recent years regarding the use of vaginal mesh, particularly when used in prolapse surgery. This is because we now know that some women may develop complications from this surgery which can significantly affect their quality of life. These complications are infrequent but affected women brought political pressure to bear, aided by social media, resulting in an Australian Senate Enquiry which reported its findings in 2017. Affected women also began a legal class action against one of the main mesh manufacturers (J&J) which was recently successful. As a result of such litigation, and the Senate Enquiry, the Australian TGA (Therapeutic Goods Administration) has withdrawn licencing for mesh products used for prolapse surgery. Many pelvic surgeons feel that this is unfortunate, as there are some women who would benefit from having these products available as an option for their symptomatic and often recurrent prolapse.
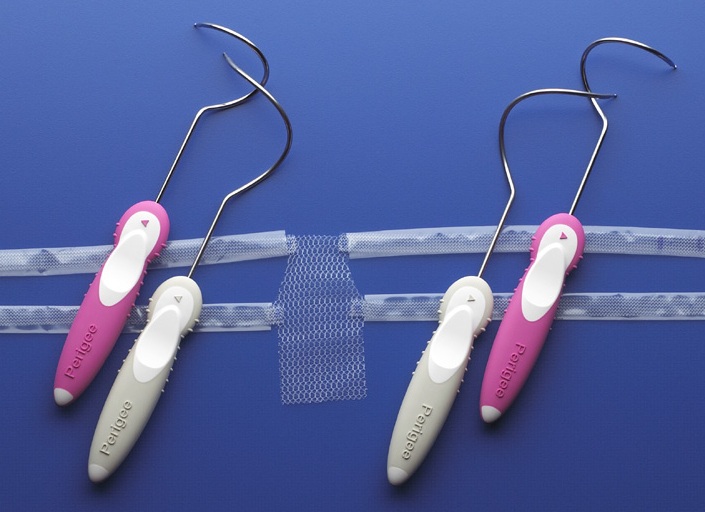
A mesh kit for anterior vaginal prolapse.
Polypropylene material has also been used frequently in the last 15 years for the surgical treatment of female urinary stress incontinence. This is called a mid urethral sling or tape. A 1cm width polypropylene sling is placed under the mid urethra through a small vaginal incision. This is often a day surgery procedure and has excellent success rates and very low morbidity. Most Urogynaecologists and pelvic surgeons feel that the advent of the mid urethral slings has been one of the major advances in women’s health in the last fifty years. The previous most common procedure was the Burch Colposuspension, which often required up to a week in hospital and six weeks recovery. Although any surgical procedure can be associated with complications, these are very uncommon with the mid urethral slings. They remain available in Australia and are the current Gold Standard procedure for female stress urinary incontinence in most countries around the world.
Mid Urethral Slings
These minimally invasive procedures were first introduced in Australia in 1998 and rapidly replaced other operations for female urinary stress incontinence. The quick recovery from this procedure and its low morbidity and high success rate, also resulted in many older women having surgery for their stress incontinence, who would not have done so with the bigger procedures. There is extensive data to support the use of mid urethral slings, with over two thousand scientific publications, making this the most extensively investigated continence procedure ever. The partners of SUC have performed research on sling surgery since 1998 with colleagues in New Zealand, Melbourne, Sydney, Canberra, Brisbane and Townsville. We have also run training courses for gynaecologists in how to perform mid urethral sling surgery.
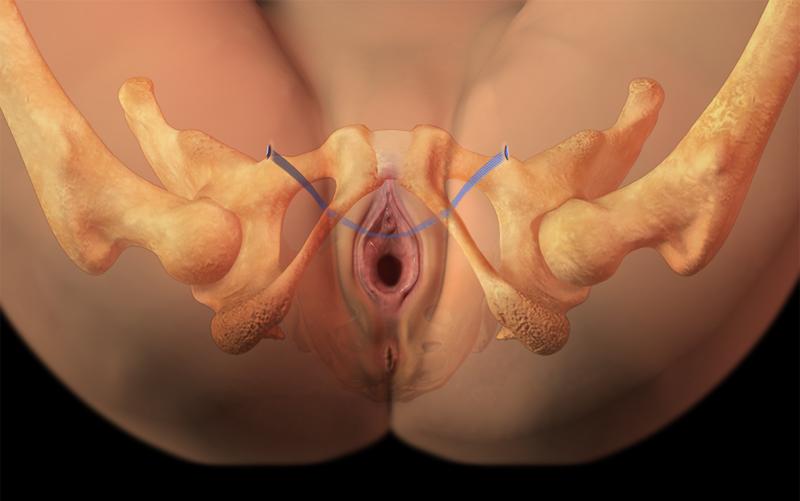
A success rate of around 90% can be expected when performed as a primary procedure. These slings can be inserted by either a retropubic (the tape passes behind the pubic bone) or transobturator approach. In the latter procedure, the tape exits in the groin. Both approaches work well for most women. However, the different approaches have different risks and benefits and their use depends on patient factors and the surgical experience and preference of the surgeon. The mid urethral slings have less risks than most other available continence procedures and equal or better success rates. Common MUS devices include the TVT and TVT Exact (retropubic) and TVT-O (transobturator). Another popular sling was the Monarc but this is no longer available.
A Trans obturator mid urethral sling (TVT-O)
Possible complications from mid urethral sling surgery
– Bleeding
– damage to the bladder or urethra
– voiding difficulties
– urge incontinence
– pain, discomfort with intercourse
– mesh exposure (~ 2%)
– bowel or blood vessel perforation
Many women with bladder problems have both stress and urge incontinence. The mid-urethral slings are designed to treat stress incontinence but often help urge leakage as well. However, this cannot be guaranteed. The slings are permanent implants and in most women the benefit is long lasting. The procedure can be repeated but this is rarely required.
The use of mid urethral slings for urinary stress incontinence is supported by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG), The International Urogynaecological Association (IUGA), the Urogynaecological Society of Australasia and the American Urogynaecological association (AUGS). In fact, the Australian Commission on Safety and Quality in Health Care has the midurethral tape (polypropelene) as the preferred option for surgical management of Stress Urinary Incontinence. See https://www.safetyandquality.gov.au/our-work/transvaginal-mesh/resources/.
The partners at Sydney Urodynamic Centres have extensive experience in the insertion of mid urethral slings by both approaches, and have inserted many thousands of slings and continue to believe that this is the procedure is of choice for most women with significant urinary stress incontinence who requires surgery. We are also able to offer other options for the surgical treatment of stress incontinence if these are indicated or requested. These options include fascial slings, colposuspensions, and the use of periurethral bulking agents. Urodynamic studies prior to surgery are recommended in order to confirm the diagnosis and exclude other conditions such as voiding disorders and detrusor overactivity.
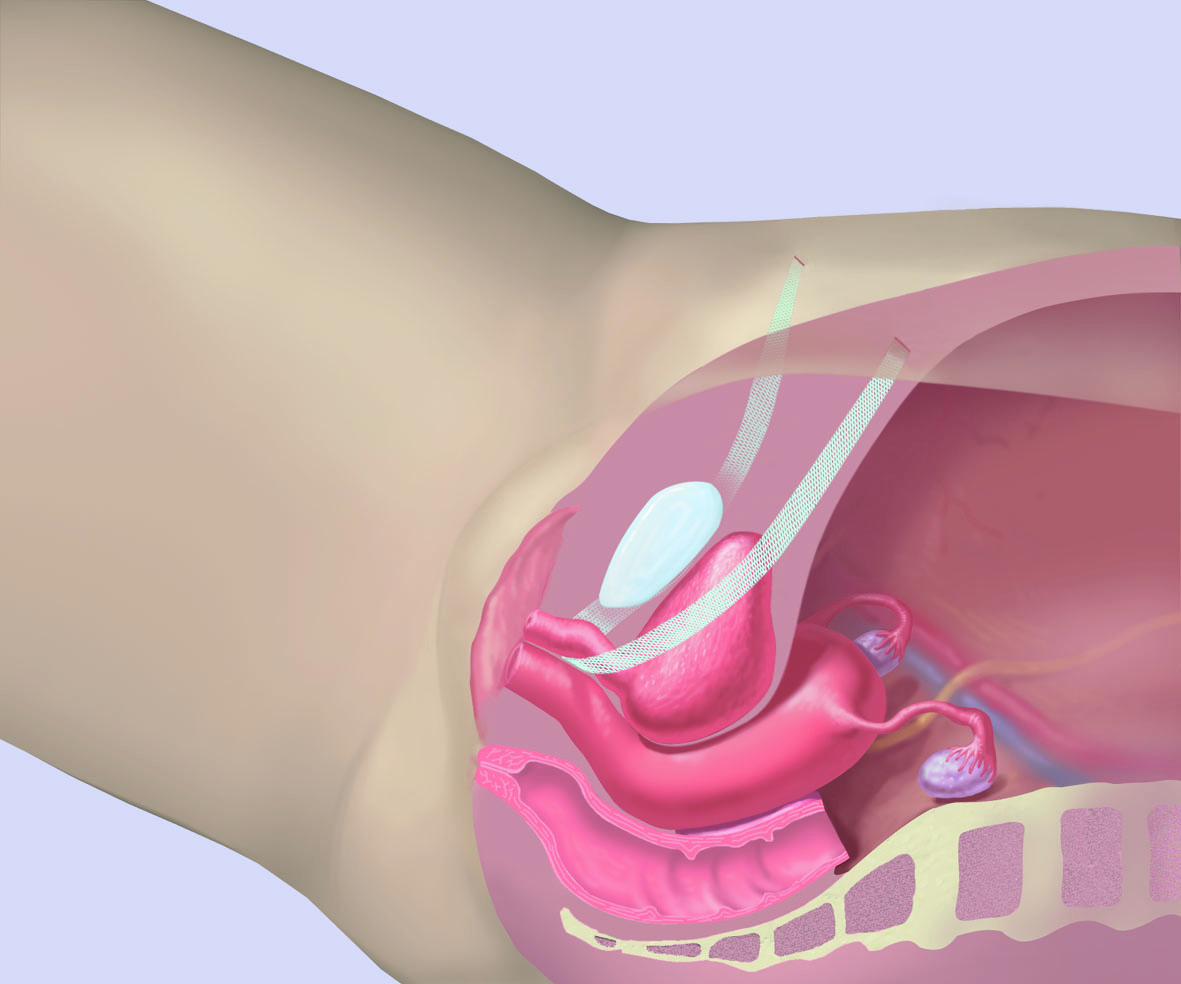
A TVT mid urethral sling (retropubic)
Vaginal Mesh procedures for Prolapse
There have been many different mesh devices made by a number of different companies and designed to treat different types of prolapse. These are attached to different anatomical structures and by a variety of techniques. These procedures have been performed in Australia since 2004 with peak usage in 2010. It is estimated that 25,000 women in Australia have had prolapse surgery with the mesh being used (approximately 11% of vaginal prolapse repairs). In the USA in 2011, 23% of vaginal repairs utilized mesh.
It is difficult to obtain accurate information on complications, however, the UK and Australian data both indicate a rate of moderate or severe adverse events occurring in less than 1% of women having trans vaginal mesh surgery. This compares well with other types of surgery.
Possible complications from vaginal Mesh Surgery
– mesh erosion (where mesh fibres protrude through the vaginal skin)
– chronic pain
– discomfort with intercourse
– vaginal discharge or bleeding
– adverse effects on urinary or bowel function
It is important to note that the vast majority of women who have had transvaginal mesh surgery have not experienced these complications and on longer follow-up remain very satisfied with their management. The partners of SUC have performed research on mesh surgery since 2004, involving over 1000 women and in collaboration with colleagues in Melbourne, Sydney, Brisbane and Townsville.
Management of Vaginal Mesh Complications
Mesh ‘erosions’ are the most common complication. These are often asymptomatic but may cause bleeding or discomfort with intercourse. They often resolve with vaginal estrogen cream but may need minor surgery. Mesh erosion occurs in 8-10% of women who have had vaginal mesh inserted. Severe or chronic pain can occur following transvaginal mesh surgery and can be debilitating. Fortunately, this is very infrequent. Referral to a Pain management team is worthwhile. Occasionally a patient may need partial or complete removal of the mesh. This is complex surgery and should only be performed by experienced pelvic surgeons. There are such surgeons in Australia who can do these procedures and there is no need for women to travel overseas as some have done. Unfortunately, complete resolution of pain symptoms is not commonly achieved by mesh removal. This is complicated by the fact that chronic pelvic pain due to other causes is common in women.
Most capital cities in Australia now have clinics available for the management of women with concerns or problems related to vaginal mesh surgery. In Sydney, these are at RPAH, Nepean Hospital, Westmead Hospital, St George Hospital, and RNSH. The partners at Sydney Urodynamic Centres also have considerable experience in managing these problems. If you wish to discuss these matters in consultation with one of the partners this can be arranged by phoning 02 97906969.
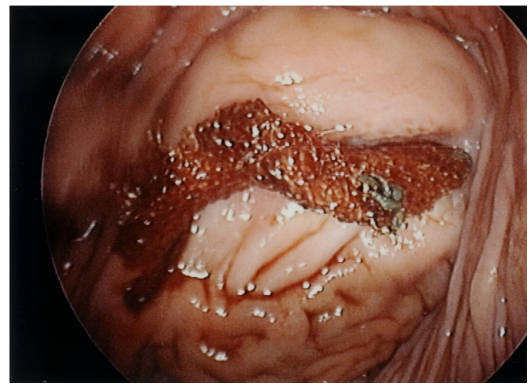
A vaginal mesh erosion on anterior vaginal wall
Surgical Training
As with all surgical procedures, adequate supervised training should be obtained in the particular surgical technique to be performed or device inserted. Mid urethral sling insertion should only be undertaken by those regularly carrying out these procedures. All of the partners at Sydney Urodynamic Centres have many years of experience in performing mid urethral slings.
Abdominal Sacrocolpopexy
This is a surgical procedure for prolapse of the vaginal vault which can occur after a woman has had a hysterectomy. Polypropylene mesh is attached to the top of the vagina (via an abdominal incision or with key hole surgery) and then secured to the sacral promontory. It is an excellent procedure for vault prolapse with good longterm success and remains a common procedure in Australia. It appears that mesh placed in the abdomen, such as in this procedure, has a much lower risk of complications than mesh inserted vaginally. The Australian Commission on Safety and Quality in Health Care has the Abdominal Colposacropexy, using polypropylene mesh, as the preferred option for the surgical management of vaginal vault prolapse.
https://www.safetyandquality.gov.au/our-work/transvaginal-mesh/resources/.
Fig indicating the mesh placement in an abdominal colposacropexy
Mesh Registry
A registry of surgical procedures and their complications is very helpful, particularly when new devices are introduced into surgical practice. This did not occur for the introduction of transvaginal mesh procedures for prolapse or for the mid urethral slings. This lack of clinical governance was noted by the Senate Enquiry and is now being addressed with a national vaginal mesh registry.



https://urodynamic.com.au/urodynamic-webblog/vaginal-mesh/trackback/